Giant granules in white blood cells
A 33 years old female suffering from recurrent bacterial and fungal infections was moved from a local nursing home to our palliative care unit because of increasingly inadequate food and fluid intake due to severe painful fungal and herpes stomatitis. The evident immune-deficient patient presented ocular albinism, congenital nystagmus and mental retardation. Laboratory analyses showed slight anemia (hemoglobin (7.6 mmol/L)), leukocytopenia (2.77 × 109/L) due to absolute neutropenia (0.5 × 109/L), decreased electrolytes, highly elevated C-reactive protein (CRP) (128 mg/L), elevated IgG (18.5 g/L), markedly increased gamma-glutamyltransferase (286 U/L) and alkaline phosphatase (220 U/L). Liver enzymes and renal function were inconspicuous. Platelets were within the lower normal range (179 × 109/L).

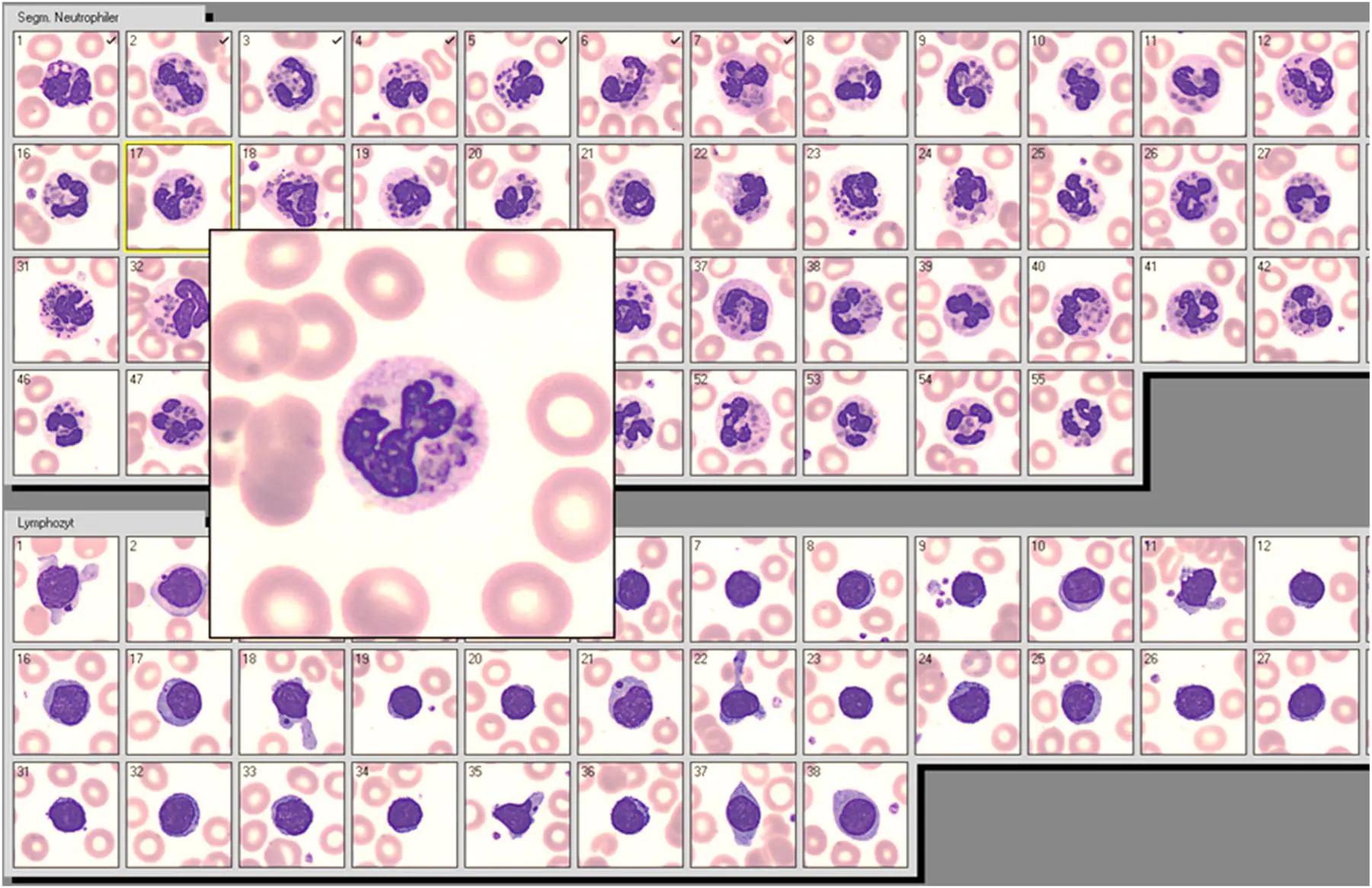
The routine WBC differential was performed by automated digitalized microscopy (Cellavision™, Sysmex Europe, Norderstedt, Germany), showing a series of leukocytes with multiple characteristic cytoplasmic inclusions and lymphocytes with giant azurophil granules.
This autosomal recessive inherited syndrome of deficient innate immunity due to misdistribution of myeloperoxidase was first observed by Beguez-Cesar [1] and further described by Chediak, a Cuban hematologist [2], and Higashi, a Japanese pediatrician [3]. This explains the designation of the disease as Chediak-Higashi-Syndrome (CHS).
The molecular basis is the mutation of the LYST/CHS1 gene located at chromosome 1 [4]. The gene product, a highly conserved cytosolic protein (“lysosomal trafficking regulator”), is differently expressed in all cell types [5].
There is no specific treatment, except allogeneic hematological stem cell transplantation (HSCT). The here presented case of the syndrome, which normally leads to premature death within the first two decades of life [6] was far accelerated at admission, receiving palliative care until death 17 days later.
According to the literature, the giant WBC inclusions are the most reliable clinical diagnostic criterion of CHS (see Figure 1), which might be overlooked in conventional blood films of CHS patients with typical neutropenia [7]. Automated digital microscopy allows the careful review of more than hundred neutrophils displayed simultaneously; thus facilitating the detection of characteristic cellular inclusions. Digital microscopy might be therefore advantageous for rapid diagnosis of CHS in the hematological routine.
Corresponding author: Peter Schuff-Werner, Institute of Clinical Chemistry and Laboratory Medicine, Rostock University Medical Center, Schillingallee 35, 18057 Rostock, Mecklenburg-Western Pomerania, Germany, E-mail: pschuffw@web.de
Original Paper/Full Text:
Schuff-Werner, Peter and Junghanss, Christian. „Giant granules in white blood cells“ Journal of Laboratory Medicine, vol. 49, no. 2, 2025, pp. 94-95. https://doi.org/10.1515/labmed-2025-0033
Meistgelesen
 Hantavirus aktuell: Nachweis, Symptome, Therapie Was ist das Hantavirus? Hantaviren sind eine Gruppe von Viren, die weltweit vorkommen und vor allem...
Hantavirus aktuell: Nachweis, Symptome, Therapie Was ist das Hantavirus? Hantaviren sind eine Gruppe von Viren, die weltweit vorkommen und vor allem...- Hantavirus: Fakten statt Panik Meldungen über drei Todesfälle im Zusammenhang mit einem Hantavirus-Ausbruch auf dem Kreuzfahrtschif...
- Hantavirus: Experten der Universitätsmedizin Essen sehen geringes Risiko für die Allgemeinbevölkerung Nachdem es auf dem Kreuzfahrtschiff „Hondius“ zu mehreren Hantavirus-Infektionen und Todesfällen gek...